Post-Acute Pressure Injury Care: When to Add dHACM
Clinical case series demonstrates durable closure of year-long pressure injuries using adjunctive dehydrated human amnion chorion membrane in home-based wound care.
Damon Ebanks
Medipyxis
Medical education note: This article is for clinicians and is not a substitute for patient-specific medical advice.
Key Takeaways
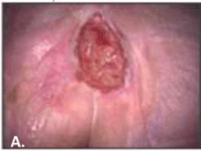
 Patient with sacral pressure injury at initial visit — chronic for over one year.
Patient with sacral pressure injury at initial visit — chronic for over one year.
Who & Where: Two elderly patients with multi-morbid conditions and pressure injuries lasting over one year transitioned from hospital outpatient care to home-based mobile wound care.
What Changed: After standard care including serial debridement and compression therapy failed to progress wounds, clinicians introduced dehydrated human amnion/chorion membrane (DHACM; EpiFix®) applied weekly to biweekly.
Outcomes: Both wounds achieved durable closure within four months under the mobile care protocol.
Why It Matters: Post-acute patients face heightened recurrence risk due to advanced age, reduced mobility, and multiple medications. Integrating DHACM into post-acute workflows may resolve long-standing pressure injuries when conservative approaches alone prove insufficient.
Why Focus on Post-Acute Pressure Injuries Now?
In 2023, approximately 323,000 Medicare beneficiaries filed roughly 900,000 claims for pressure injury treatment. Many patients discharge before achieving durable closure or experience recurrence, then cycle through long-term hospitals, inpatient rehabilitation, skilled nursing facilities, or home-based care—settings where limited mobility and polypharmacy elevate risk. A mobile wound care team documented two patients whose year-long pressure injuries finally closed after introducing DHACM in the home setting.
What the Team Did
Setting & Tracking
- Mobile clinicians followed patients in their homes after prior hospital outpatient care
- Each visit documented treatments, wound characteristics, and size measurements to track progress
Foundational Care First
- Continued standard care: debridement; compression when indicated
- Identified a "stall" when appropriate fundamentals failed to improve wound area or bed quality
Adjunctive Biologic
 Same patient — pressure injury closed after 4 months of treatment with adjunctive DHACM.
Same patient — pressure injury closed after 4 months of treatment with adjunctive DHACM.
- Initiated DHACM (EpiFix®) at weekly–biweekly intervals until closure
- Achieved time to closure within four months for both long-standing pressure injuries
Clinical Implications for Wound Programs
1) Make the Post-Acute Handoff Intentional
Treat discharge as the midpoint rather than the finish line. Patients with advanced age, low mobility, and multiple comorbidities face greater recurrence risk and may benefit from proactive escalation pathways in home or skilled nursing facility settings.
2) Use DHACM as an Adjunct After a True Stall
This series applied DHACM only after consistent debridement and compression failed to produce progress, aligning with an "adjunctive after-stall" strategy rather than initial-line substitution.
3) Expect Pragmatic Cadence
The team applied DHACM weekly to biweekly, reassessing bed quality and size at each encounter—a simple, repeatable approach compatible with mobile workflows.
A Simple Post-Acute Workflow You Can Pilot
-
Re-baseline at First Post-Acute Visit
- Confirm pressure injury staging, measure area, document bed quality
- Continue debridement; apply compression when indicated
-
Define "Stall"
- No meaningful progress despite fundamentals over a reasonable interval
-
Add DHACM
- Apply weekly–biweekly; maintain photo and area trends to verify effectiveness
-
Stay Mobile-Care Friendly
- Build a cadence fitting home visits and caregiver capacity
-
Declare Success
- Continue until durable closure; plan recurrence prevention and follow-up
Strengths, Limits, and Stakeholder Communication
Strengths: Real-world post-acute and home-based context; practical application cadence; closure of year-long pressure injuries within four months after adding DHACM.
Limitations: Small sample (n=2), single program experience; not a comparative study; one author affiliation with the DHACM manufacturer (MIMEDX) noted—interpret with appropriate caution.
Bottom Line for Leadership: In carefully selected stalled pressure injuries, adjunctive DHACM integrated into post-acute protocols may shorten closure timelines and reduce readmissions after discharge.
FAQ
What is DHACM and how was it used here?
DHACM (dehydrated human amnion/chorion membrane; EpiFix®) represents a placental-derived biologic used here as an adjunct to standard PI care after a stall, applied weekly to biweekly in the home until closure.
Did DHACM Replace Debridement or Compression?
No. Debridement and compression continued throughout; DHACM was added only when conservative therapy alone failed to generate progress.
How Fast Did the Wounds Close?
Both year-long pressure injuries achieved durable closure within four months after adding DHACM in the mobile care program.
Why Emphasize Post-Acute and Home-Based Care?
Older, less mobile, multi-morbid patients discharged from hospitals face heightened non-closure or recurrence risk. A structured post-acute plan with escalation pathways can address this critical gap.
Bottom Line
For post-acute patients with stalled, year-long pressure injuries, adding DHACM to sound fundamentals in a home-based mobile care model coincided with closure within four months in this small series. Consider establishing a defined escalation pathway to DHACM once conservative therapy reaches a true plateau in the post-acute setting.
References
- EPUAP/NPIAP/PPPIA 2019 Clinical Practice Guideline: Prevention and Treatment of Pressure Ulcers/Injuries. EPUAP
- AHRQ: Preventing Pressure Ulcers in Hospitals (burden & cost). AHRQ
- Berhane CC et al., 2019. dHACM for pressure ulcer treatment: case series. J Wound Care. Mag Online
- Serena TE et al., 2022. Multicenter RCT of dHACM + compression in chronic VLUs. Wound Rep Reg. PMC
- NICE MIB139: EpiFix for chronic wounds; weekly application. NICE
- Wiley Wound Repair Regen 2023: Risk factors for pressure ulcer recurrence. Wiley
- Narayan N et al., 2025. RCT: dHACM vs collagen-based substitute in Stage III–IV pressure ulcers. PubMed