Bioactive Glass Matrix for Hydroxyurea Leg Ulcers
71-year-old polycythemia vera patient achieved rapid healing of three medication-induced ankle ulcers using weekly bioactive glass matrix applications.
Damon Ebanks
Medipyxis

Medical education note: This article is for clinicians and is not a substitute for patient-specific medical advice.
Problem
Up to 10–15% of patients on hydroxyurea develop cutaneous toxicity, including painful, non-healing ulcers often complicated by multiple medications and age-related conditions.
Patient
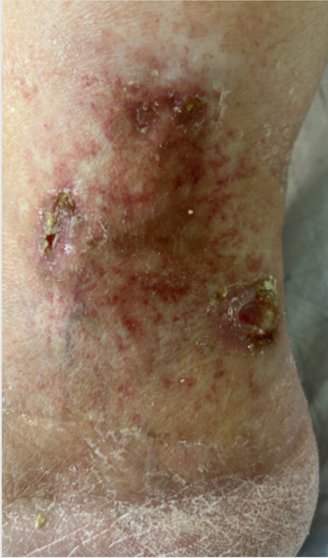
 71-year-old male with three hydroxyurea-related clustered ulcers on the right medial ankle.
71-year-old male with three hydroxyurea-related clustered ulcers on the right medial ankle.
A 71-year-old male presented with three clustered ulcers on the right medial ankle related to hydroxyurea therapy.
Intervention
Weekly borate-based bioactive glass fiber matrix (BBGFM) was applied following sharp debridement, covered with self-adaptive gauze and wrapping. Treatment involved serial tracking of length, width, depth, wound bed quality, and exudate levels.
Outcomes
 Week 2 healing progress.
Week 2 healing progress.
- Wound 1: Reduced from 1.80 cm³ to complete closure by week 6
- Wound 2: Progressed from 0.14 cm³ to closure by week 5
- Wound 3: Approached near-closure by week 7
 Week 7 healing progress.
Week 7 healing progress.
Implication
BBGFM may overcome medication-related healing barriers by delivering a pro-angiogenic, pro-granulation scaffold, potentially counteracting hydroxyurea's cytotoxic effects on skin cells and blood vessel formation.
Why These Ulcers Are Difficult to Close
Hydroxyurea's chronic exposure triggers refractory ulcers through:
- Reduced keratinocyte and fibroblast proliferation
- Blunted new blood vessel formation and microvascular damage
- Systemic anti-inflammatory effects from additional medications
Mechanism of Borate-Based Glass
The matrix releases therapeutic ions (boron, calcium, phosphorus) that support new blood vessel development, fibroblast activation, and an antimicrobial environment.
Clinical Guidance
Triage: Screen polycythemia vera patients for hydroxyurea-associated ulcers and document all medications.
Treatment Protocol: Sharp debridement → bioburden control → apply BBGFM → protect with self-adaptive gauze and wrap; reassess weekly.
Tracking Signals: Early volume reduction by week 2 and closure by weeks 5–6 align with published bioactive glass outcomes.
Multimodal Care: Compression therapy, offloading, and moisture balance remain essential alongside matrix application.
Limitations
Single-patient case without control group; causality cannot be definitively established. However, time-bound closures and photo-verified epithelialization represent clinically meaningful signals.
References
- Hydroxyurea-related ulcer BBGFM case. SAWC Fall 2025.
- Sirieix ME, et al. Leg Ulcers and Hydroxyurea: Forty-one Cases. Arch Dermatol. 1999.
- Armstrong DG, et al. Resorbable glass microfiber matrix vs SOC. Int Wound J. 2021.