Squamous Cell Carcinoma from Pilonidal Disease: Marjolin Ulcer Case
Clinical guide on recognizing squamous cell carcinoma transformation in pilonidal disease with case report and practical diagnostic workflow.
Damon Ebanks
Medipyxis
Medical education note: This article is for clinicians and is not a substitute for patient-specific medical advice.
Clinical takeaway: When a pilonidal wound stalls or evolves—biopsy early. Delays can allow malignant change (Marjolin ulcer) to progress and complicate care.
Why This Matters
Squamous cell carcinoma developing in long-standing pilonidal disease is rare (~0.1%) but potentially devastating. It can masquerade as a "routine" nonhealing sinus, leading to missed or delayed diagnoses.
Case in Brief
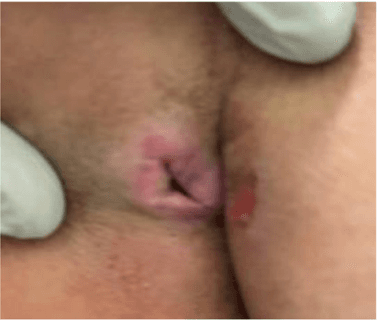
 Squamous cell carcinoma initial visit — note the frond-like, friable, bleeding edges characteristic of Marjolin ulcer.
Squamous cell carcinoma initial visit — note the frond-like, friable, bleeding edges characteristic of Marjolin ulcer.
- Patient: 38-year-old woman with a longstanding mass of the left upper buttock and history of pilonidal disease.
- Course before diagnosis: Four months of continuous drainage from a ruptured mass; referral to surgery was missed due to scheduling barriers. Re-presentation months later revealed a vertically aligned, fissure-like, full-thickness wound 3–4 cm deep with irregular, frond-like edges that bled easily and possible sacral bone involvement.
- Diagnosis & plan: Pathology returned squamous cell carcinoma infiltrating the reticular dermis. Patient was referred to surgical oncology for complete excision. Given wound depth and concern for expansive local disease/regional spread, neoadjuvant therapy was considered.
- System lens: A five-month gap existed between initial presentation and the wound-care visit; during this interval she visited the ED twice without a tissue diagnosis, and the wound length increased from ~3 cm to ~6 cm.
Marjolin Ulcer: The Historical Pattern You Can Still Spot at the Bedside
The term Marjolin ulcer dates to 1828 (Jean Nicolas Marjolin). Classic descriptions include villous/fungating projections, a firm granular texture or red, friable tissue that bleeds easily—features that mirror the frond-like, bleeding edges observed in this case.
Red Flags for SCC in Pilonidal Disease
Consider urgent biopsy when you see any of the following:
- Persistent drainage or nonhealing after months of care.
- Fissure-like, full-thickness tract with 3–4 cm depth or more.
- Irregular, frond-like/cauliflowering edges that bleed easily.
- Rapid change in size (e.g., 3 cm → 6 cm over months).
- Location consistent with pilonidal sinus and a longstanding mass that "ruptured."
- Possible bone involvement (clinical concern for sacral penetration).
Pearl: "If a wound is not healing, biopsy it." This principle applies with special urgency to chronic pilonidal disease.
Practical Workflow
1) Reassess the "Chronic Pilonidal Wound"
Document size, depth, edge morphology, bleeding on contact, drainage, and pain; review duration and prior episodes of abscess/rupture. If red flags are present, do not delay biopsy.
2) Biopsy Strategy
Sample the edge and base to capture invasive fronts; avoid superficial curettage that yields only inflammatory debris.
3) While Awaiting Pathology, Stabilize the Wound
The team used dilute sodium hypochlorite (Dakin's)–soaked packing with a foam dressing, a reasonable bridge to control bioburden and exudate without macerating the tract.
4) Positive Result? Stage and Refer Quickly
The reported plan was complete surgical excision with consideration of neoadjuvant therapy given lesion depth and risk of regional spread.
5) Close the Loop on System Barriers
Establish fast-track pathways for suspicious wounds to prevent multi-month diagnostic delays.
What Clinicians Should Learn From This Case
- Transformation is uncommon but real. SCC arising in pilonidal sinus disease occurs at an estimated ~0.1% rate.
- Edge architecture matters. Frond-like, friable, or easily bleeding borders are classic malignant clues.
- Delays worsen the field. In just a few months, this wound doubled in length.
- A simple rule prevents misses: Biopsy any chronic, nonhealing pilonidal wound—especially after rupture.
Bottom Line
In chronic pilonidal disease, don't normalize a wound that keeps changing. The combination of deep fissuring, bleeding frond-like edges, interval growth, and persistent drainage should prompt immediate biopsy and expedited oncologic management—before the window for a less morbid operation closes.
References
- Michalopoulos N, et al. Squamous cell carcinoma arising from chronic sacrococcygeal pilonidal disease. World J Surg Oncol. 2017.
- Iqbal FM, Sinha Y, Jaffe W. Marjolin's ulcer: a rare entity with a call for early diagnosis. BMJ Case Rep. 2015.
- Shah M, Crane JS. Marjolin Ulcer. StatPearls. 2023.
- Pekarek B, et al. A Comprehensive Review on Marjolin's Ulcers. J Am Col Certif Wound Spec. 2012.
- Khan K, et al. Marjolin Ulcer: A Comprehensive Review. Adv Skin Wound Care. 2020.
- Pandey MK, Gupta P, Khanna AK. Squamous cell carcinoma arising from pilonidal sinus. Int Wound J. 2012.