Massive Localized Lymphedema: Panniculectomy Resolves Chronic Wounds
Panniculectomy with advanced surgical techniques achieves durable wound closure and restored mobility in morbidly obese patients with MLL.
Damon Ebanks
Medipyxis

Medical education note: This article is for clinicians and is not a substitute for patient-specific medical advice.
Why Massive Localized Lymphedema Matters in Wound Care
Massive localized lymphedema (MLL) represents an increasingly recognized complication in severely obese patients, characterized by huge, pendulous masses of lymphedematous tissue that drag on the ground and create chronic skin breakdown. These lesions resist conventional wound management because the underlying problem is mechanical and lymphatic rather than superficial.
What Is Massive Localized Lymphedema?
MLL manifests as a benign soft-tissue overgrowth, typically on the lower extremities, abdomen, or genital region in morbidly obese individuals. The condition develops slowly over years, with histology showing chronic lymphedema, fibrotic tissue, and adipose overgrowth. Patients often face misdiagnosis as soft-tissue sarcoma due to the mass's size and firmness.
Why Panniculus-Associated Wounds Become Chronic
The tissue underside creates a perfect storm for chronic wounds: constant moisture, occlusion, friction, and poor air circulation. Maceration breaks the skin barrier, allowing bacterial and fungal colonization. Combined with lymphatic insufficiency and the mechanical shear from pannus weight, even advanced dressings cannot achieve durable closure.
Case Snapshots
Case 1
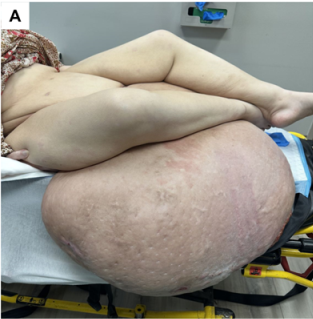 32-year-old woman with morbid obesity and an abdominal pannus over 112 cm in length and weighing 194 lb.
32-year-old woman with morbid obesity and an abdominal pannus over 112 cm in length and weighing 194 lb.
A 32-year-old woman with a 194-pound abdominal pannus measuring over 112 centimeters in length became confined to nursing-home care with bilateral thigh wounds and severe hip dysfunction. Conservative therapy could not control chronic drainage.
Case 2
 60-year-old woman with a 12.5-lb right thigh pannus and recurrent panniculitis.
60-year-old woman with a 12.5-lb right thigh pannus and recurrent panniculitis.
A 60-year-old woman with a 12.5-pound right thigh pannus experienced recurrent panniculitis, frequent falls, and chronically draining wounds despite standard wound care and antibiotics.
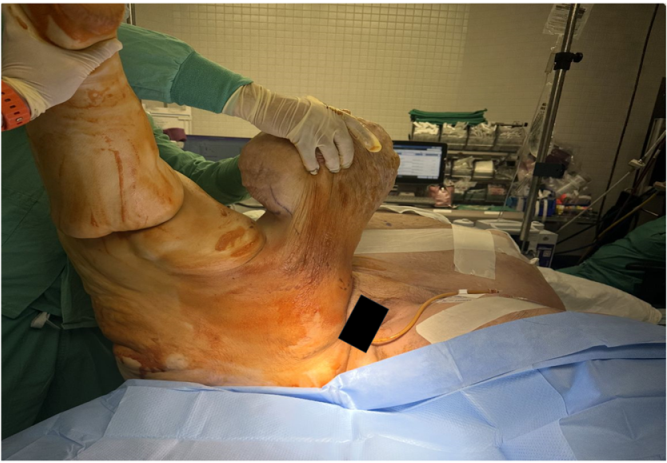
Surgical Strategy: Panniculectomy as Definitive Wound Care
Both patients underwent panniculectomy with wide excision of devitalized tissue followed by complex local flap closure. This approach removes the pathologic tissue causing obstruction and mechanical trauma.
Intraoperative Adjuncts
- Pure hypochlorous acid irrigation for bioburden reduction
- Progressive tension sutures (PTS) to minimize dead space and distribute tension
- Incisional negative pressure wound therapy (iNPWT) over closed incisions
- Closed-suction drains to evacuate fluid while compressive garments support stability
Outcomes
 Case 1 patient outcome — restored mobility after panniculectomy.
Case 1 patient outcome — restored mobility after panniculectomy.
Case 1 achieved primary closure with only minor groin dehiscence, healing conservatively. The patient was discharged home ambulatory and independent after previously residing full-time in nursing facility care.
 Case 2 patient outcome — stable ambulation regained.
Case 2 patient outcome — stable ambulation regained.
Case 2 underwent closure of a 546 square-centimeter thigh defect using local flap techniques, recovering without complications and regaining stable ambulation.
Recognizing Panniculectomy Candidates in Wound Clinic
Red-flag patterns include:
- Massive pannus enlarging over years in morbidly obese patients
- Recurrent panniculitis or cellulitis despite adequate therapy
- Progressive functional decline preventing independent ambulation, bathing, or self-care
- Multiple prior wound-care "failures" where the underlying problem is clearly mechanical
Early plastic or reconstructive surgery consultation is appropriate when these features appear.
Bottom Line
MLL represents an under-recognized driver of chronic panniculus wounds and severe functional impairment in obese patients. Conservative wound care alone rarely cures MLL-related wounds because the core pathology is mechanical and lymphatic. Carefully planned panniculectomy with advanced techniques and multidisciplinary support achieves durable wound closure and dramatic improvements in mobility.
References
- Massive localized lymphedema and panniculectomy case series. SAWC Fall 2025.
- Bujang-Safawi E, et al. Massive localized lymphedema. Lymphat Res Biol.
- Progressive tension sutures in abdominoplasty. Plast Reconstr Surg.
- Incisional NPWT for high-risk closures. Int Wound J.