Hydroxyurea-Associated Heel Ulcer in PV and Diabetes: ON101 Case
67-year-old with polycythemia vera on hydroxyurea and diabetes healed 9-month chronic heel ulcer in 14 days using ON101 topical cream.
Damon Ebanks
Medipyxis

Medical education note: This article is for clinicians and is not a substitute for patient-specific medical advice.
Why This Case Matters (1-Minute Summary)
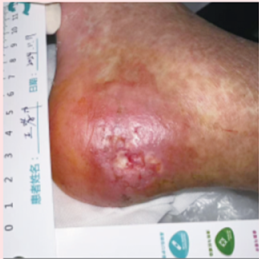 Chronic heel ulcer in diabetic patient on hydroxyurea, initial visit.
Chronic heel ulcer in diabetic patient on hydroxyurea, initial visit.
A patient with polycythemia vera (PV) on long-term hydroxyurea and type 2 diabetes developed a chronic left-heel ulcer persisting 9 months despite 5 months of growth-factor gel and petroleum dressings. Vascular workup showed normal results (ABI 1.10; angiography showed no significant stenosis), and neurological exam was unremarkable. Treatment with ON101 topical cream once daily with dry gauze resulted in rapid epithelialization by day 10 and near-complete closure by approximately day 14, using less than one tube without adverse events.
The clinical signal suggests that in PV patients who must continue hydroxyurea, a topical supporting epithelial regeneration may prevent prolonged nonhealing and avoid the difficult choice of discontinuing disease-modifying therapy.
The Backstory: PV, Hydroxyurea, and Ulcers
Hydroxyurea serves as a mainstay in PV treatment, yet chronic lower-extremity ulcers are recognized—though uncommon—complications that can become refractory to standard dressings and topical growth factors. Coexisting diabetes introduces additional microvascular and metabolic barriers, compounding the challenge. In overlap cases, clinicians often face a dilemma: discontinue hydroxyurea (risking hematologic instability) or search for a topical that can restart epithelialization without systemic side effects.
Case Snapshot
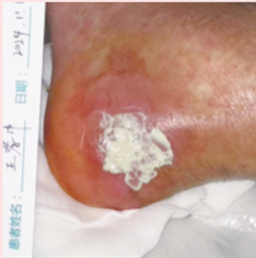 ON101 being applied to patient.
ON101 being applied to patient.
Patient: 67-year-old male; PV on long-term hydroxyurea; 9-year history of type 2 diabetes with fasting glucose 5–7 mmol/L (approximately 90–126 mg/dL).
Ulcer: Shallow heel ulcer, 9 months duration; no improvement after 5 months of growth-factor gel and petroleum-based dressings.
Workup: ABI 1.10; lower-extremity angiography negative for arterial stenosis; neurologic exam unremarkable.
Intervention: ON101 applied daily; covered with dry gauze.
Outcome: Rapid epithelialization by day 10; near-complete closure by approximately day 14, with less than one tube used; no adverse events; sustained closure on follow-up.
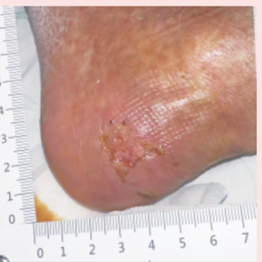 Rapid epithelialization of left chronic heel ulcer by day 10.
Rapid epithelialization of left chronic heel ulcer by day 10.
Practical Lessons for Wound Clinics
1) Confirm (and Document) That the Basics Are Optimized
- Perfusion: Normal ABI and angiography here ruled out ischemia as the rate-limiter. Address vascular disease first if present.
- Infection control, cleanse, and cover: Continue evidence-based cleansing and moisture-balanced coverage while introducing any new topical.
- Systemic factors: Glycemic control in this patient was reasonable; optimize HbA1c and nutrition in parallel.
2) Think "Drug-Related Ulcer" in PV on Hydroxyurea
Hydroxyurea-associated ulcers are widely described and can be stubborn; they often push teams toward discontinuation. A safe, effective topical that triggers epithelial regeneration may avoid systemic changes and support closure—even in complex comorbidity stacks.
3) Consider ON101 as an Adjunct When Standard Topicals Stall
What stood out here was speed (epithelialization by day 10; near-closure by approximately day 14) and tolerability (no reported adverse events), despite prior failure with growth-factor therapy.
Suggested Clinic Protocol
Patient selection: PV on hydroxyurea ± diabetes; chronic ulcer greater than 8–12 weeks; perfusion adequate (e.g., ABI ≥0.9 and/or definitive imaging); no progressive infection.
Topical course: ON101 once daily to wound surface, cover with dry gauze. Continue offloading and standard peri-wound protection.
Monitoring: Photograph at baseline and every 3–4 days; track surface area and epithelial migration.
Escalation: If no response by 2–3 weeks, reassess for occult infection, pressure/offloading gaps, or systemic barriers.
Limitations
This is a single case with strong visual and timeline documentation but no control arm; generalizing efficacy, dose-response, or recurrence risk to broader PV or diabetic populations is not possible.
Bottom Line
When a hydroxyurea-associated leg ulcer stalls despite good fundamentals—and ischemia and infection are ruled out—a time-limited trial of ON101 may be a pragmatic, low-risk adjunct. In this PV and diabetes case, that approach was followed by visible epithelial advance within 10 days and near-complete closure in approximately 2 weeks, with sustained healing on follow-up.
References
- Dissemond J, et al. Hydroxyurea-induced ulcers on the leg. Dtsch Arztebl Int. 2009.
- Sirieix ME, et al. Leg Ulcers and Hydroxyurea: Forty-one Cases. Arch Dermatol. 1999.
- Huang YY, et al. Effect of a Novel Macrophage-Regulating Drug (ON101) on Wound Healing in DFUs—Phase 3 RCT. JAMA Netw Open. 2021.
- McMullin MF, et al. BSH Guideline: Diagnosis and management of polycythaemia vera. Br J Haematol. 2019.
- Aboyans V, et al. Measurement and Interpretation of the Ankle-Brachial Index. Circulation. 2012.