GV/MB PVA & PU Foams for ECF Wounds: Case-Based Protocol
Post-Whipple enterocutaneous fistula management using gentian violet-methylene blue foam dressings with documented healing over four months.
Damon Ebanks
Medipyxis
Medical education note: This article is for clinicians and is not a substitute for patient-specific medical advice.
Why Enterocutaneous Fistula Wounds Are So Brutal
Major abdominal surgery complicated by intra-abdominal sepsis and enterocutaneous fistula (ECF) hits the trifecta of wound-care misery: high bioburden, relentless effluent, and a periwound that's constantly under chemical attack. ECFs carry significant risks of prolonged hospitalization, malnutrition, sepsis, and elevated mortality rates.
The Case: Post-Whipple Abdominal Wound With Enterocutaneous Fistula
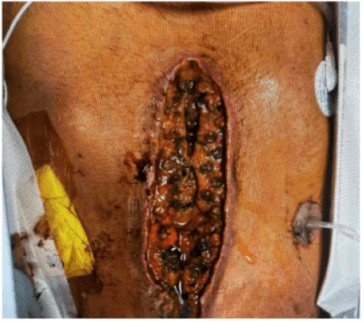
 100% granular tissue with exposed muscle and sutures exposed with ECF.
100% granular tissue with exposed muscle and sutures exposed with ECF.
Following pancreaticoduodenectomy, a patient developed intra-abdominal abscesses requiring multiple surgical washouts, eventually resulting in a large abdominal defect with continuous fistula drainage. Treatment goals included controlling infection, managing heavy exudate, protecting fragile periwound tissue, and stabilizing the wound during systemic recovery.
A wound manager system isolated the fistula. The primary treatment strategy employed gentian violet/methylene blue-impregnated PVA and PU foams. Over approximately four months, the wound demonstrated significant size reduction and robust granulation while the fistula remained contained.
What Makes Gentian Violet–Methylene Blue Foam "Blue Magic"?
Broad-Spectrum Antimicrobial Action With Low Toxicity
These organic dyes provide non-cytotoxic, broad-spectrum antibacterial coverage against gram-positive bacteria, gram-negative organisms, and yeast—including resistant strains. The binding within foam matrices enables sustained antimicrobial delivery without relying on silver or iodine compounds.
Foam Structure for Exudate Handling and Comfort
PVA micro-pore foam requires hydration before application, becoming soft and flexible to wick and retain fluid while maintaining intimate wound contact.
PU foams offer high absorptivity and conform to irregular surfaces, making them suitable as wounds shallow and drainage moderates.
How the Dressing Strategy Worked in This Case
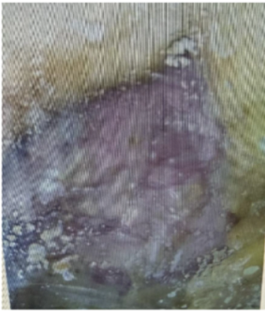 Wound healing progression after 4 months with repeated application of GV/MB dressing.
Wound healing progression after 4 months with repeated application of GV/MB dressing.
1. Isolate the Fistula, Protect the Skin
A dedicated wound manager contained effluent and diverted output away from the wound bed and periwound tissue, aligning with fistula best-practice protocols.
2. PVA GV/MB Foam for the Early "Messy" Phase
Early wound management required intensive bioburden control, high-capacity exudate handling, and a contact layer that wouldn't adhere to fragile tissue.
3. PU GV/MB Foam as the Wound Shallowed
As granulation filled the wound and drainage moderated, transition to polyurethane foam provided comfort, flexibility, and strong exudate management while maintaining antimicrobial coverage.
Practical Tips for Using GV/MB Foams in Complex Abdominal Wounds
- Stabilize the patient first. Sepsis management, nutrition, and fluid-electrolyte status require active intervention before topical dressings become effective.
- Pair foam dressings with fistula isolation. Wound managers, ostomy appliances, or pouching systems keep effluent away from the wound bed.
- Match foam type to wound phase. Deeper, wetter, contaminated wounds benefit from GV/MB PVA foam. Shallower, granulating wounds with moderate drainage suit GV/MB PU foam.
- Watch for early success indicators. Decreased odor, cleaner wound beds, reduced slough, and improved granulation quality.
- Keep the approach individualized. Success derives from willingness to adapt dressing selection.
Bottom Line
Enterocutaneous fistula after major abdominal surgery creates one of the most challenging wound-care environments. Gentian violet/methylene blue foam dressings combine broad-spectrum antimicrobial activity with fluid-handling benefits of PVA and PU foams.
In this post-Whipple case, alternating GV/MB-impregnated PVA and PU foams alongside a wound manager produced substantial wound contraction and granulation over four months despite fistula presence and prior intra-abdominal sepsis.
References
- GV/MB PVA & PU foams for ECF case. SAWC Fall 2025.
- Edwards K, et al. Gentian Violet and Methylene Blue Antibacterial Foams. PMC.
- Hydrofera Blue Product Monograph.
- ECF management consensus guidelines. Surg Clin North Am.