Fish Skin Before STSG: Staged DFU Reconstruction
Two-stage surgical approach using acellular fish-skin graft followed by split-thickness skin graft for chronic diabetic foot ulcers.
Damon Ebanks
Medipyxis

Medical education note: This content is for clinicians and does not replace device IFUs or institutional protocols.
Quick Take
For chronic, non-healing diabetic foot ulcers (DFUs) resistant to conservative management, a two-stage surgical strategy—acellular fish-skin graft (FSG) to optimize wound bed quality, followed by split-thickness skin graft (STSG)—demonstrated uniformly complete graft take, rapid wound healing, and no major postoperative infections or graft failures in a UT Health San Antonio series.
Why Stage DFU Closure?
STSG success depends critically on wound-bed quality. In compromised beds—common in diabetes due to ischemia, neuropathy, and bioburden—graft take is suboptimal and healing prolonged. Piscine-derived acellular fish-skin, rich in omega-3 fatty acids and intact extracellular matrix, served as a bioactive scaffold to stimulate granulation and vascularized tissue, creating a graft-receptive surface before STSG.
Who Was Treated & How It Worked
 Patient with complex foot ulcer, initial visit.
Patient with complex foot ulcer, initial visit.
- Population: Adults with chronic, non-healing DFUs that failed meticulous local wound care and off-loading.
- Stage 1 – Prepare & prime the bed: Sharp debridement of devitalized tissue, then application of acellular fish-skin to the wound base. Clinicians waited for healthy granulation and visible FSG incorporation.
- Stage 2 – Definitive cover: Once the bed appeared ready, clinicians performed STSG.
Outcomes That Matter to Limb-Salvage Teams
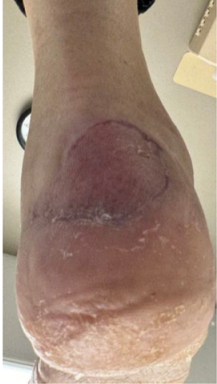 Diabetic foot ulcer four weeks into healing after acellular fish skin graft.
Diabetic foot ulcer four weeks into healing after acellular fish skin graft.
- Graft take: Complete in each patient; no graft failures.
- Complications: No major postoperative infections; no FSG-related adverse events.
- Function: Baseline or improved ambulatory status at follow-up; minimal donor-site morbidity.
- Speed: Authors report rapid wound healing and reduced healing time compared with historical DFU trajectories.
Practical Playbook: FSG → STSG
- Debride decisively. Remove all nonviable tissue; manage infection and optimize perfusion.
- Apply fish-skin graft. Ensure conformal contact with the wound base; protect with secondary dressings and maintain off-loading.
- Wait for "integration signals." Look for robust granulation and visible FSG incorporation before scheduling STSG.
- Perform STSG. Proceed once the bed is uniformly vascular and free of slough or gross bioburden.
- Rehab & surveillance. Continue off-loading, glucose control, and serial assessments.
Why This Approach Can Help Your Service
- Biology before coverage: FSG provides a bioactive scaffold that upgrades bed quality, improving STSG uptake in high-risk DFUs.
- Fewer setbacks: The series saw no major postoperative infections or graft failures.
- Functional focus: Maintaining (or improving) ambulation matters as much as closure.
Limitations
This is an early, single-team experience without a control group. While findings are promising, the authors call for larger comparative studies to validate timing, patient selection, and cost-effectiveness.
Bottom Line
In high-risk DFUs, fish-skin grafting to prime the wound bed followed by STSG is a pragmatic staged pathway that yielded reliable graft take, fast healing, and no major complications—while maintaining patient mobility.
References
- Zhao Y, Shen QQ. Acellular fish skin grafts in diabetic foot ulcer care: meta-analysis and clinical insights. World J Diabetes. 2025.
- McCartan B, et al. The Use of Split-Thickness Skin Grafts on Diabetic Foot Ulcerations. Eplasty. 2012.
- Gao J, et al. Efficacy of acellular fish skin graft in chronic ulcers: meta-analysis. 2024.
- Dardari D, et al. Intact fish skin graft vs standard of care in diabetic foot wounds. Medicina. 2022.
- IWGDF Offloading Guideline 2023.
- IWGDF/IDSA 2023 Infection Guideline.