Continuous Topical Oxygen Therapy: 5 Real-World Cases
Five complex chronic wounds—surgical dehiscence, burns, osteoradionecrosis—achieved complete closure using continuous topical oxygen as adjunct.
Damon Ebanks
Medipyxis

Medical education note: This article is for clinicians and is not a substitute for patient-specific medical advice.
Chronic Wounds Go Far Beyond DFUs and VLUs
A 2017 economic evaluation found that chronic nonhealing wounds affect roughly 8.2 million Medicare beneficiaries, costing up to $96.8 billion annually. Many of these wounds extend beyond classic diabetic foot ulcers (DFUs) and venous leg ulcers (VLUs)—including surgical wounds that dehisce, traumatic injuries, and complex ulcers. Notably, these wound types remain underrepresented in randomized controlled trials, creating an evidence gap that real-world case data can help address.
What Is Continuous Topical Oxygen Therapy (cTOT)?
Topical oxygen therapy delivers oxygen directly to the wound surface, typically under an occlusive or semi-occlusive dressing, rather than systemically. In continuous topical oxygen therapy, a low-flow stream of humidified oxygen supplies the wound bed for extended periods, creating a high-oxygen microenvironment that supports:
- Collagen synthesis and fibroblast proliferation
- Angiogenesis and capillary budding
- Bacterial control and biofilm disruption
- Enhanced epithelial cell migration
Case Series: Five Diverse Chronic Wounds Closed With cTOT
Case 1 – Surgical Wound Dehiscence After Fasciotomy
 39-year-old male with surgical wound dehiscence after fasciotomy (72 cm²).
39-year-old male with surgical wound dehiscence after fasciotomy (72 cm²).
- Patient: 39-year-old male, New York, USA
- Etiology: Surgical wound dehiscence following radical fasciotomy
- Baseline size: 72.0 cm²
- Outcome: Complete closure in 77 days with cTOT
Case 2 – Full-Thickness Burn of the Thigh
 41-year-old female with full-thickness burn on thigh (28 cm²).
41-year-old female with full-thickness burn on thigh (28 cm²).
- Patient: 41-year-old female, Pretoria, South Africa
- Outcome: Complete closure in 84 days with cTOT
Case 3 – Osteoradionecrosis Extending to the Mandible
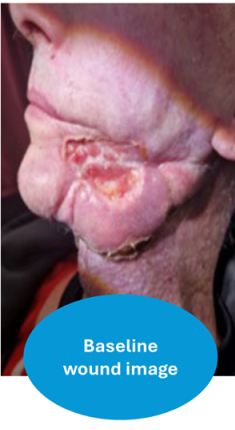 65-year-old male with osteoradionecrosis extending to the mandible.
65-year-old male with osteoradionecrosis extending to the mandible.
- Patient: 65-year-old male, Luton, UK
- Outcome: Complete closure in 35 days of cTOT
Case 4 – Sternotomy Dehiscence Post-Cardiac Surgery
 72-year-old male with sternotomy dehiscence post-cardiac surgery.
72-year-old male with sternotomy dehiscence post-cardiac surgery.
- Patient: 72-year-old male, Porto, Portugal
- Outcome: Complete closure in 26 days of cTOT
Case 5 – Calciphylaxis Wound
 56-year-old female with calciphylaxis wound.
56-year-old female with calciphylaxis wound.
- Patient: 56-year-old female, Cleveland, USA
- Outcome: Complete closure in 64 days of cTOT
Across these five cases—spanning surgical dehiscence, burns, osteoradionecrosis, sternotomy, and calciphylaxis—continuous topical oxygen served as an adjunct to standard care and was associated with full closure in clinically meaningful timeframes.
How Do These Results Fit the Broader Evidence?
A 2023 systematic review and meta-analysis found that topical wound oxygen therapy, compared with standard care alone, significantly increased the probability of complete healing and shortened time to closure in chronic diabetic foot ulcers. The IWGDF 2023 guideline recommends considering topical oxygen therapy as an adjunct for DFUs when standard care alone has not achieved healing.
Clinical Considerations for Using cTOT
1. Confirm and Optimize Perfusion First
Topical oxygen is not a substitute for revascularization in critical limb-threatening ischemia. Before initiating cTOT, assess macrocirculation and microcirculation.
2. Debride Aggressively and Protect the Scaffold
All five cases received standard wound-bed preparation, including debridement and moisture-balanced dressings, before and during cTOT.
3. Use cTOT as an Adjunct, Not a Standalone
The most robust data support cTOT layered on top of best standard of care—offloading, infection control, exudate management, and optimization of systemic issues.
4. Think Beyond DFUs and VLUs
These data highlight potential value of cTOT in dehisced surgical wounds, complex burns, osteoradionecrosis, and calciphylaxis—wound types underrepresented in randomized trials.
5. Choose Patients Who Can Adhere to Continuous Therapy
Continuous devices require wearing a small oxygen delivery unit and maintaining an adequate seal at the wound interface.
Bottom Line
Chronic nonhealing wounds represent a massive burden—and many are not classic DFUs or VLUs. These five cases align with a growing body of evidence supporting topical oxygen therapy as a safe and effective adjunct in chronic wounds. For wound programs, cTOT is a practical, outpatient-friendly tool to consider when standard care stalls.
References
- Five real-world cTOT cases (international case series).
- IWGDF 2023 Wound-Healing Interventions Guideline.
- Topical wound oxygen therapy for chronic DFUs: 2023 systematic review.
- Economic burden of chronic wounds. 2017.