Bioactive Glass Matrix for Complex Leg Wounds: 4-Case Series
Borate-based bioactive glass fibrous matrix shows substantial healing improvements in four refractory lower-extremity wounds, including complete DFU closure.
Damon Ebanks
Medipyxis

Medical education note: This article is for clinicians and is not a substitute for patient-specific medical advice.
Quick Take
A clinician case series using a borate-based bioactive glass fibrous matrix (BBGFM) on four difficult lower-extremity wounds reported substantial percent-area reduction (PAR) across all cases and complete closure in one diabetic foot ulcer—after standard care had failed. Applications ranged from one to seven, over 5–13 weeks, with PAR from 70.96% to 100%.
Study at a Glance
Design & setting. Four patients with complex lower-extremity wounds received BBGFM as an adjunct to standard care. Primary endpoint: percent area reduction (PAR).
Case 1: Pyoderma Gangrenosum
 Patient with pyoderma gangrenosum, initial visit.
Patient with pyoderma gangrenosum, initial visit.
Case 2: Venous Leg Ulcer with Hematoma
 Venous leg ulcer with hematoma.
Venous leg ulcer with hematoma.
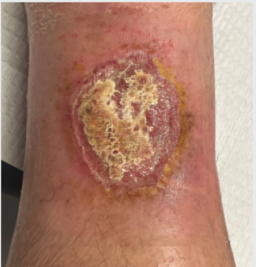
Case 3: Necrotizing Fasciitis (Post-Debridement)
 Necrotizing fasciitis, initial visit.
Necrotizing fasciitis, initial visit.
Case 4: Wagner 3 Diabetic Foot Ulcer
 Patient with Wagner 3 diabetic foot ulcer.
Patient with Wagner 3 diabetic foot ulcer.
Results
- PG: 7 applications over ~13 weeks → 70.96% PAR
- VLU/hematoma: 1 application over ~11 weeks → 92.46% PAR
- Necrotizing fasciitis: 1 application over ~7 weeks → 90.16% PAR
- DFU: 2 applications over ~5 weeks → 100% PAR (full closure)
 PG wound after 12 weeks of healing.
PG wound after 12 weeks of healing.
 DFU fully closed after 5 weeks of treatment.
DFU fully closed after 5 weeks of treatment.
Interpretation: BBGFM functioned as a bioactive skin-substitute scaffold across inflammatory (PG), vascular (VLU), infectious (post-NF), and diabetic wounds. The complete DFU closure underscores its potential as an adjunct in high-risk, previously non-healing wounds.
Why Borate-Based Bioactive Glass?
- Antimicrobial support: A 2023 in-vitro study showed BBG matrices reduced a broad panel of 19 wound-relevant pathogens for up to 7 days.
- Pro-angiogenic signaling: Borate-based glass fibers stimulate VEGF under dynamic flow conditions.
- Soft-tissue compatibility: Reviews highlight expanding soft-tissue applications for bioactive glasses beyond bone.
- Clinical momentum: A multicenter RCT compared a resorbable glass microfiber matrix to collagen–alginate in DFUs, supporting superior outcomes with the glass matrix at 12 weeks.
How to Use BBGFM (Practical Protocol)
1) Prepare the Bed
Perform sharp debridement to a bleeding surface; address infection per standard of care. Optimize offloading (DFU/heel) or compression (VLU) when arterial supply allows.
2) Place the Matrix
Fill and cover the defect with the fibrous matrix; ensure uniform contact. Moisten with sterile saline per manufacturer instructions to initiate handling and conformability.
3) Dress & Maintain
Use a moisture-balanced secondary dressing; set change intervals to wound status. Reassess weekly to biweekly; track PAR to verify trajectory.
4) Combine Thoughtfully
Continue standard care (edema control, glycemic management). BBGFM in the series was adjunctive, not a replacement for standard of care.
Where It Fits in Your Algorithm
Reassess at 4–6 weeks of standard care. If stalled, consider BBGFM for:
- Venous ulcers with persistent exudate/hematoma
- Postinfectious cavities after necrotizing fasciitis debridement
- Neuropathic DFUs with chronicity despite hyperbaric oxygen therapy/advanced dressings
Pair with fundamentals: offloading/compression, infection control, glycemic optimization. Measure and document PAR; escalate or add adjunctive therapies (e.g., NPWT, grafts) if trajectory is suboptimal.
Bottom Line
For refractory lower-extremity wounds—including DFU, VLU, PG, and post-NF defects—a borate-based bioactive glass fibrous matrix can be a useful adjunct to standard care. In a small series, all cases improved substantially by PAR, and a chronic DFU closed completely within five weeks after two applications.
References
- BBGFM 4-case series for complex leg wounds. SAWC Fall 2025.
- Armstrong DG, et al. Resorbable glass microfiber matrix vs SOC. Int Wound J. 2021.
- Ren Z, et al. Bioactive Glasses: Advancing Skin Tissue Repair. 2025.
- BBG antimicrobial activity against wound pathogens. 2023.